
US healthcare: most people don't know what they're talking about
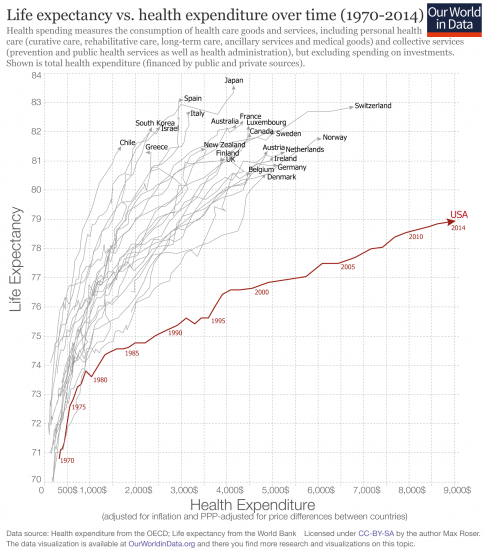
US healthcare is famous for three things: it's expensive, it's not universal, and it has poor outcomes. The US spends around $7,000 per person on healthcare every year, or roughly 18% of GDP; the next highest spender is Switzerland, which spends about $4,500. Before Obamacare, approx 15% of the US population were persistently uninsured (8.6% still are). And as this chart neatly shows, their overall outcome on the most important variable—overall life expectancy—is fairly poor.
But some of this criticism is wrongheaded and simplistic: when you slice the data up more reasonably, US outcomes look impressive, but being the world's outrider is much more expensive than following behind. What's more, most of the solutions people offer just don't get to the heart of the issue: if you give people freedom they'll spend a lot on healthcare.
The US undoubtedly spends a huge amount on healthcare. One popular narrative is that because of market failures and/or extreme overregulation in healthcare, prices are excessively high. So Americans with insurance (or covered by Medicare, the universal system for the elderly, or Medicaid, the government system for the poor) get the same as other developed world citizens, but those without get very poor care and die younger. A system like the NHS solves the problem, according to this view, with bulk buying of land, labour, and inputs, better incentives, and universal coverage.
But there are some serious flaws in this theory. Firstly, extending insurance to the previously-uninsured doesn't, in America, seem to have large benefits. For example, a recent NBER paper found no overall health gains from the massive insurance expansion under Obamacare.* A famous RAND study found minuscule benefits over decades from giving out free insurance to previously uninsured in the 1970s. In fact, over and above the basics, insuring those who choose not to get insurance doesn't ever seem to have large gains. Indeed, there is wide geographic variation in the life expectancy among the low income in the US, but this doesn't even correlate with access to medical care! This makes it unlikely that the gap between the US and the rest is explained by universality.
To find the answer, consider the main two ingredients that go into health outcomes. One is health, and the other is treatment. If latent health is the same across the Western world, we can presume that any differences come from differences in treatment. But this is simply not the case. Obesity is far higher in the USA than in any other major developed country. Obviously it is a public health problem, but it's unrealistic to blame it on the US system of paying for doctors, administrators, hospitals, equipment and drugs.
In fact in the US case it's not even obesity, or indeed their greater pre-existing disease burden, that is doing most of the work in dragging their life expectancy down; it's accidental and violent deaths. It is tragic that the US is so dangerous, but it's not the fault of the healthcare system; indeed, it's an extra burden that US healthcare spending must bear. Just simply normalising for violent and accidental death puts the USA right to the top of the life expectancy rankings.

{kind=link}
{kind=link}
This is what we'd expect if we approached the topic more honestly, and dug into the detail of healthcare stats. You might think—you might think!—that this is what international healthcare rankings like those from the WHO or the Commonwealth Fund do. Not so. The WHO just looks at a corrected life expectancy measure, but not one corrected for any of the factors which attempt to isolate the impact of healthcare. The Commonwealth Fund's is a mix of high level aggregate measures like physicians per capita and a survey asking people around the world questions like whether "Doctor or other clinical staff talked with patient about a healthy diet and healthy eating". Neither are useless, but they are not the real deal.
Academic papers that drill down into the detail find that the US does well in cancer survival, heart attack and stroke survival, and successfully medicating those with long-term conditions such as diabetes. In fact, when the Commonwealth Fund did this sort of analysis themselves decades ago, the US ranked among the best of countries. This is partly because the US has much more advanced equipment, partly because it funds more costly treatments in general, and partly because it funds the newest treatments, when their marginal costs are often stratospheric. This may subsidise medical research for everyone else.
Now this is not to say the US system works well. The fact that the US spends vastly more than everyone else, and only does a bit better, if that, makes the system pretty unimpressive. But it's important to understand why. The UK really does have "death panels" that refuse treatments because they're extremely costly relative to their tiny impact. The USA has a system where most people can buy—are even subsidised through the tax system to buy—insurance that is as extensive as they like, paying for ever more expensive and marginally beneficial therapies. Eventually you're spending a fifth of your GDP on it.
Maybe if the US government straightened things out—scrapped the incentives that push people to get too much healthcare and deregulated the system to increase competition and push down costs the US would spend a more rational share of its income on health. I think this is pretty likely. But I bet the gap wouldn't go away fully. Americans just have a lot of cash, and want to spend an increasing share of it on their wellbeing as they get even richer. As long as the system is mostly open, I'd expect that to continue.
*see tables 3, 7, and 8 for subsample analysis; doesn't look like any sub-group has seen any significant gains at all