Healthcare Tim Worstall 08/10/2015 Healthcare Tim Worstall 08/10/2015 We would blame central heating ourselves Read More Healthcare Tim Worstall 07/10/2015 Healthcare Tim Worstall 07/10/2015 The best part of Britain's health care Read More Healthcare Tim Worstall 02/10/2015 Healthcare Tim Worstall 02/10/2015 So how much should the world's fifth largest economy pay toward drug development? Read More Healthcare Tim Worstall 18/09/2015 Healthcare Tim Worstall 18/09/2015 Now we've won, let's kill what works! Read More Healthcare Tim Worstall 16/09/2015 Healthcare Tim Worstall 16/09/2015 Can we get this straight please? Obesity saves the NHS money Read More Healthcare Tim Worstall 12/09/2015 Healthcare Tim Worstall 12/09/2015 What good news as we face more First World Problems Read More Healthcare Holly Mackay 11/09/2015 Healthcare Holly Mackay 11/09/2015 The Assisted Dying Bill should not have been euthanised Read More Healthcare Tim Worstall 05/09/2015 Healthcare Tim Worstall 05/09/2015 Another societal mass delusion, this time about sugar Read More Healthcare Tim Worstall 04/09/2015 Healthcare Tim Worstall 04/09/2015 So that's the end of minimum pricing on booze then Read More Healthcare Tim Worstall 23/08/2015 Healthcare Tim Worstall 23/08/2015 Good grief, this is ridiculous Read More Healthcare Tim Worstall 15/08/2015 Healthcare Tim Worstall 15/08/2015 Somewhat ghoulish but interesting all the same Read More Healthcare Tim Worstall 04/08/2015 Healthcare Tim Worstall 04/08/2015 If you think for profit health care is expensive wait until you see not for profit... Read More Newer Posts Older Posts Your subscription could not be saved. Please try again. Your subscription has been successful. Blogs by email Enter your email address to subscribe I agree to receive your newsletters and accept the data privacy statement. SUBSCRIBE
Healthcare Tim Worstall 08/10/2015 Healthcare Tim Worstall 08/10/2015 We would blame central heating ourselves Read More
Healthcare Tim Worstall 07/10/2015 Healthcare Tim Worstall 07/10/2015 The best part of Britain's health care Read More
Healthcare Tim Worstall 02/10/2015 Healthcare Tim Worstall 02/10/2015 So how much should the world's fifth largest economy pay toward drug development? Read More
Healthcare Tim Worstall 18/09/2015 Healthcare Tim Worstall 18/09/2015 Now we've won, let's kill what works! Read More
Healthcare Tim Worstall 16/09/2015 Healthcare Tim Worstall 16/09/2015 Can we get this straight please? Obesity saves the NHS money Read More
Healthcare Tim Worstall 12/09/2015 Healthcare Tim Worstall 12/09/2015 What good news as we face more First World Problems Read More
Healthcare Holly Mackay 11/09/2015 Healthcare Holly Mackay 11/09/2015 The Assisted Dying Bill should not have been euthanised Read More
Healthcare Tim Worstall 05/09/2015 Healthcare Tim Worstall 05/09/2015 Another societal mass delusion, this time about sugar Read More
Healthcare Tim Worstall 04/09/2015 Healthcare Tim Worstall 04/09/2015 So that's the end of minimum pricing on booze then Read More
Healthcare Tim Worstall 23/08/2015 Healthcare Tim Worstall 23/08/2015 Good grief, this is ridiculous Read More
Healthcare Tim Worstall 15/08/2015 Healthcare Tim Worstall 15/08/2015 Somewhat ghoulish but interesting all the same Read More
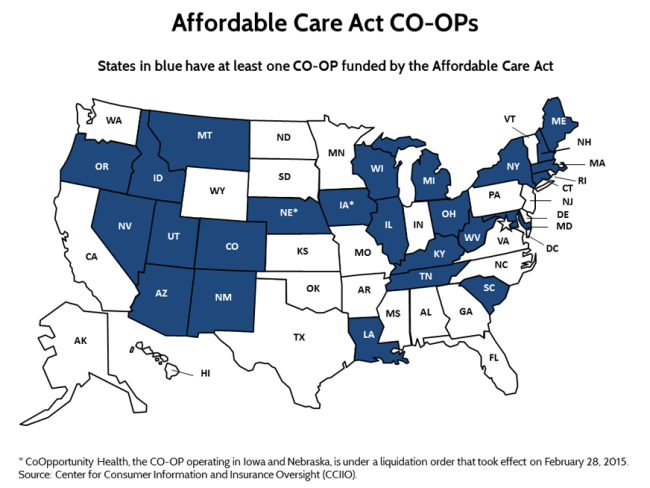
Healthcare Tim Worstall 04/08/2015 Healthcare Tim Worstall 04/08/2015 If you think for profit health care is expensive wait until you see not for profit... Read More