

Bitcoin and the Beeb
Crypto-currencies such as Bitcoin have already changed the way we pay for things. For a start, it speeds payments up. Instead of institutions like banks controlling our money, it is now issued independently – with thousands of bitcoin miners trying to discover more.
But it is still rather clunky. All those bitcoin-mining computers whirring away consume vast amounts of energy. And it is still, in a sense, centralised. New generations of programmable money will be more efficient and more dispersed still. And that will change the way we pay for things yet again.
With micro-payments of a tiny fraction of a cent becoming easy-peasy, they will also become routine. Why endure TV ads, for example, when you can simply pay a tiny amount online to watch ad-free content?
Which might completely change our thinking about the BBC. The government is about to issue its thoughts on the corporation's future, and other technological changes (such as the relative ease with which we can now operate subscription systems) might change it fundamentally, even if the government doesn't. But just think about how micro-payments could change public broadcasting even further. Most of the BBC's content is pure entertainment. And bolted on are some 'public service' functions, like current affairs programmes. (That is why politicians love it - they get to watch Newsnight and other tedious political content.)
In a world of micro-payments, your TV can charge you for watching the entertainment and (if that is really what the politicians insist on), not charge you for the boring Newsnight. But think further. Who would really want ads on the commercial channels when you can pay - a tiny amount - not to have them? Or could we actually be looking at a world in which the BBC takes adverts in return for being 'free', and the commercial channels are ad-free, at least to those who pay a bit?
The possibilities are endless. Which is another good reason why the BBC should not be a public monopoly.

Sure, there's such a thing as market failure
Much as it pains to admit it there really is something called market failure. Markets are not perfect - only very good. We would note that most of what people call market failures - say Lord Stern's argument that climate change is the largest such ever - are not in fact failures at all. They are absences. Markets don't deal with externalities, whether positive or negative, because as that word externality implies, they are outside markets.
But even given that it is true that markets are not the appropriate solution to everything. However, we also need to know that there's such a thing as government failure. It's no good our shouting that markets have failed thus that bloke with a Third in PPE from Gradgrind Poly must know how to deal with it. It's possible that there simply isn't a solution to the problem. It's also entirely possible that government will be worse at whatever the task is:
The SNP has admitted that the new IT system set up to deliver common agricultural policy (Cap) payments to farmers is “not there yet”.
Fergus Ewing, rural economy secretary, told MSPs that arrangements for the payment of 2016 subsidies were “not risk-free” as he announced that eligible farmers and crofters would be able to apply for a loan of up to 80 per cent of the value of their entitlement.
Mr Ewing confirmed that by last Friday 17,744 out of 18,479 eligible businesses had received their 2015 payments, with “the majority of outstanding cases” expected to be paid by the October 15 deadline.
The traditional measure of competence is the ability to organise a piss up in a brewery. Here we have government unable to give away free money - not even rising to that modest measure, is it?
Markets might not be able to solve every problem in this vale of tears that is human existence: but it's remarkable how few of them government is able to deal with.

But who will build the roads?
Ed Glaeser is one of the most interesting economists in the world at the moment, thanks to his iconoclastic work on the economics of cities. I think some of his approach can be summed up as looking at cities at things that grow or emerge spontaneously, and can't be constructed (or stimulated) by the government into growth.
His latest essay for City Journal focuses on infrastructure spending, which some people seem to view as a sort of panacea – it stimulates the economy, and you get some nice new roads! Or maybe not:
The existence of plausible transportation alternatives and the law of diminishing returns have also tended to reduce the benefits of infrastructure investment over the past two centuries. The opening of the Erie Canal in 1821 brought enormous value because the inland transportation options at the time were dismal. In the early nineteenth century, it cost as much to ship goods 30 miles over land as to send them across the entire Atlantic Ocean. Yet the very existence of canals, as much of a breakthrough as they represented, reduced the benefits of the later rail system, as Nobel economist Robert Fogel has shown. The returns for new transportation infrastructure in places with terrible roads, such as much of Africa and India, will be much higher than in the United States, which already enjoys an impressive, if under-maintained, array of mobility options.
What about the economic value of the shorter commuting times that new infrastructure can bring? Between 2009 and 2014, the Texas Transportation Institute estimates that the annual cost to Americans from traffic rose from $147 billion to $160 billion and that hours wasted in traffic increased from 6.3 billion hours to 6.9 billion hours, despite the surge in federal transportation funding. The time wasted has been particularly egregious in America’s more successful metropolitan areas, like San Jose, where delays per auto commuter jumped from 56 hours in 2009 to 67 hours in 2014. Yet it’s hard to see how substantially reducing time lost to traffic congestion will turbocharge the economy. Imagine that America gets its act together and cuts traffic time sufficiently to save $80 billion—a pretty miraculous improvement. That would still represent less than one-half of 1 percent of America’s $18 trillion GDP.
Read the whole thing.

Today's Oxfam report says increasing inequality increases inequality
We suspect that Oxfam might want to think a little bit more about this part of their report today:
Research carried out for Oxfam by the London School of Economics, to be published later this year, shows empirical evidence that poverty rates tend to be higher when inequality is higher and increases in income inequality are associated with increases in income poverty rates.
Err, yes, we suppose so.
Poverty in the UK is a relative measure. Less than 60% of median household income adjusted for household size (and often after housing costs). This is a measure of inequality, not one of poverty.
Thus the actual information content of that coming report is that increasing inequality increases inequality.
Err, yes, we suppose so really.

A first stab at explaining the surging money supply
Allister Heath is getting worried over the surging money supply. It's entirely possible that he's right to worry as well. What follows is not *the* way to think about this. It is, rather, *a* way to walk through the basics of the subject.
Think of the equation MV = PQ. Money times the velocity of circulation equals prices times quantity demanded. One way to think of monetary policy is that to try to gee up the economy we try to increase V - we do this by lowering the interest rate. Thus, hopefully, Q increases. Similarly, if P is rising, that is we've got inflation, raise interest rates so as to reduce V and thus stop the rise in P.
Again, please note that proper monetary economists will have conniption fits at this explanation. We're really trying perhaps too hard to make it simple.
We can also simplify what we mean by "money supply". M in that equation should be thought of as M0 in the national statistics. Notes and coins and central bank reserves sorta stuff. And MV can be thought of as M4, which is M0 plus all the stuff the banking system does, loans and debts and credit and so on. Again, not right but useful as an aide memoire.
Which brings us to the recent unpleasantness. Interest rates were already near or at rock bottom. But we could see that V was plummeting. We were really rather worried about a very deep recession (Q falling) and or deflation (P falling). And the solution there is to create lots more M so that MV doesn't shrink.
Which is one way of describing what QE was and is. The Bank of England makes up some more money and goes and buys stuff with it. Simple because it has made more M0, thus MV is larger than it would be if V fell but there was no increase in M.
All of which is great. But there will come a time when V returns to something like normal. and what we don't want to have is some great overhang of M which when timesed by that now resurgent V leads to massive increases in P - because it won't turn up as Q rising 20% a year, that's for sure. That's where the so far at least unmet predictions of QE causing galloping inflation come from. It presupposes that V returns to normal, of which there's no sign yet. Or, as Heath worries, perhaps there is:
Lilico provides context for this. The 14.7pc rate of increase is a new record for this statistical series, launched in 2009. Looking at an earlier and closely comparable statistical series, the strongest rate of growth in recent history was in 2006, at the height of the pre-crash madness, when the money supply surged by 12.8pc, a jump now widely understood to have been scandalously out of control.
There are other possible explanations for this. But the above is, while a scandalously simplified explanation, a possible one. Our whole aim in doing QE was to protect the economy against that fall in V. The reason it was QE rather than going out and spending the cash is because we wanted to be able to reverse the increase in the money supply (and QE has increased M0 a number of times, it's not just a small percentage increase) if, as and or when, V recovered to more normal levels.
Thus, if V has or is recovering in order to avoid that galloping increase in P we will want to reduce M. That is, reverse QE. The Bank of England will, assuming that this is the right explanation of course, sell the gilts they have and cancel the money they collect from doing so. Or, perhaps, simply not replace maturing gilts as they currently do, thus reducing their stock of gilts over time - this will have the same effect on M as the government will have to issue new gilts to the public to replace those maturing that the Bank holds.
That is, if the money supply is booming because matters monetary are getting back to normal then the answer is for matters monetary to get back to normal. QE was a response to extraordinary times and if they're leaving the stage then so should QE.

Just what is the problem with grammar schools?
We find the current furore over grammar schools to be puzzling, difficult to understand.
Take this in the Observer. They note, correctly, that Upper Bavaria has an astonishingly low youth unemployment rate of only 3.4%. They credit, correctly, the education system:
Germany’s much-admired dual education system (in which apprentices are trained jointly by employers and at specialist vocational schools) has grown in Upper Bavaria, not because it was seen as the more responsible thing to do, but because companies, unable to “buy in” a fully trained-up workforce, often had to mould the workers they needed themselves.
That education system is dual in another manner too:
The Gymnasium is designed to prepare pupils for higher education and finishes with the final examination Abitur, after grade 12, mostly year 13. The Realschule has a broader range of emphasis for intermediate pupils and finishes with the final examination Mittlere Reife, after grade 10; the Hauptschule prepares pupils for vocational education and finishes with the final examinationHauptschulabschluss, after grade 9 and the Realschulabschluss after grade 10.
Perhaps not dual then but there's a definite separation into academic and vocational streams - streams which go to different schools. And this is a much-admired system which leads to a 3.4% youth unemployment rate.
Yet mention grammars in Britain, the equivalent of those gymnasium (and common across much of central Europe too) and we are discussing the very devil, encouraging the destruction of all that is good and holy in our society.
We don't understand it. Our assumption is that it must have something to do with left wing politics - we find that's the usual explanation for beliefs entirely at variance with reality.

How to make public policy these days
The TL:DR version of how to influence public policy these days. Ride hobby horse, spout piffle, invent targets then shout loudly.
You might think we are joking but sadly not. For this is exactly what is happening over sugar.
The hobby horse is, as we have mentioned many a time, the insistence that it is sugar which is causing all that obesity out there. This cannot be true given that calorie intake and sugar intake are both down on the levels of the past. It cannot be rising consumption which is the cause as consumption hasn't been rising.
The spout piffle part is to insist that it is:
Many believe sugar is the biggest contributor to the obesity epidemic crippling the NHS, and the results, published on Friday, reignited criticism of the failure by the government to take a stronger line in its childhood obesity strategy.
It isn't, as we've been saying. The inventing targets:
Britons are advised that sugar should account for no more than 5% of daily calories, but from 2012-14, the average was 13.4% for those aged between four and 10, 15.2% among 11- to 18-year-olds, 12.3% for adults under 65 and 11.1% for those aged 65 and over, the national diet and nutrition survey (NDNS) found.
This is a particularly cute one because the target itself, that 5%, was only invented after the period being described. It was only invented last year:
Dietary sugar should account for no more than 5% of daily calories consumed, half the previous recommended limit, the UK’s official nutrition advisers have said.
Note again, it's not just that the target is entirely pulled from some nether region it's that it didn't even exist, let alone apply to, the time period being examined. And then finally the shouting louder:
The Action on Sugar chairman, Graham MacGregor, a professor of cardiovascular medicine at Queen Mary University of London, said: “Today’s NDNS data shows that children are still consuming almost three times more sugar than the daily maximum recommendation. Theresa May must urgently rethink her pathetic childhood obesity plan that lacks restrictions on the marketing of, and promotions on, products high in saturated fat, sugar and salt.
“The strategy must include the implementation of the soft drinks industry levyand a mandatory reformulation programme, as the failed responsibility deal has already proven that a voluntary system does not work.”
We're not meeting an invented target, one that we've only just invented, which shows that compulsion is required to get everyone doing as we wish.
We really don't think this is a sensible way to run a country if we're honest. If it were possible we'd insist these campaigners spend more time with their train sets - there is at least an acknowledged role for the Fat Controller there. In the absence of that being possible we feel they should best be left to howl in the wilderness - and certainly not taken seriously.

Two particularly stupid views of trade in one morning
It's rare to be treated to two pieces of stupidity about trade on the same day but here we are, the event has happened. And sadly the people in error are people who do have at least some modicum of power over our lives.
The error being made is to be mercantilist. To think that it is the exports which are the purpose of trade, the exports which make us rich. This is, as we all know, precisely the view which Adam Smith railed against that 240 years ago and Adam Smith was right. Both in what he said and in said railing. For it is, of course, the imports which make us rich, the reason we trade is to gain access to those imports.
Here is Liam Fox:
“If you want to share in the prosperity of our country, you have a duty to contribute to the prosperity of our country,” he is reported as saying, hinting that companies that do not take advantage of new export opportunities could face sanctions.
Clearly thinking that it is exporting which makes Britain rich:
He added: “We’ve got to change the culture in our country. People have got to stop thinking about exporting as an opportunity and start thinking about it as a duty — companies who could be contributing to our national prosperity but choose not to because it might be too difficult or too time-consuming or because they can’t play golf on a Friday afternoon.”
Again, exporting being equated with increasing the wealth of the nation. From the other side of the Channel we have M. Macron who is an odds on runner for the French Presidency:
British-based financial institutions must be prevented post-Brexit from selling their services in the eurozone, Emmanuel Macron, the likely progressive left candidate for the French presidency has told the Guardian.
This is the same mistake. It is to think that the British companies doing the exporting are the beneficiaries of such exports. When nothing is further from the truth. Those who benefit are the consumers who get to enjoy the imports. for that is why we do this trade thing - in order to gain access to those things which Johnny Foreigner does better or cheaper than we do. And that's the only reason we do trade too.
It gets worse:
But Macron insisted:
“The financial passport is part of full access to the EU market and a precondition for that is the contribution to the EU budget. That has been the case in Norway and in Switzerland. That is clear.” The proposal would be rejected outright by British Eurosceptics.
The insistence is that being able to sell to people is a privilege, one that a government must pay for so that businesses may do so. But this is incorrect - the benefit is to those who may buy the imports.
By not grasping the most basic point about trade M. Macron is threatening to hold the people of the European Union hostage unless some gelt is paid to the Brussels bureaucracy. He really is shouting that he'll make Europeans poorer unless the Brits give him some money. Such is the lunacy one is driven to by not understanding the basics of trade.
It has been 240 years now since the Wealth of Nations was published. We'd really rather hoped that people had grasped the point by now.

Re-dressing old wounds: The unintended consequences of NHS prescription regulations
The current system for exempting certain patients from paying for their NHS prescriptions is discriminatory, unjust and unfit for purpose. The high cost of prescription medication deters many patients from engaging consistently with treatment, increasing their risk of adverse outcomes such as strokes and heart attacks.
When Bevan introduced the NHS in 1948, his intentions were clear and noble: nobody in this country should suffer from a treatable illness or ameliorable impairment because they were too poor to afford care.
The current system for exempting certain patients from paying for their NHS prescriptions is discriminatory, unjust and unfit for purpose. The high cost of prescription medication deters many patients from engaging consistently with treatment, increasing their risk of adverse outcomes such as strokes and heart attacks.
When Bevan introduced the NHS in 1948, his intentions were clear and honourable: nobody in this country should suffer from a treatable illness or ameliorable impairment because they were too poor to afford care.
Unfortunately his advisors had under-estimated the scale of demand for health services. From every corner of the country, people emerged in droves requesting glasses, false teeth, and wondering whether they could discard their antique trusses if they had their hernias repaired surgically.
On 1st June 1952, after four years of dismayed contemplation of the rising cost of the NHS, a prescription charge of one shilling was imposed, and a charge of one pound for dental treatment.
In 1965 prescription charges were removed again, but this was again a short-lived interval and in 1968 they were reintroduced. The only difference was this time, they were not for everyone. A list of exemptions was drawn up, based on the state of medical art in 1968, and this list has remained largely unchanged since then. In 2009 there was one major addition, to exempt people suffering from cancer, but otherwise the list has been embalmed.
As is often the case with overly complex regulations, unintended consequences arise. The aim of the original list of exemptions was to ensure that people whose lives depended on regular medication should never be unable to afford that medication.
Exemptions were granted to:
- People with epilepsy needing continuous medication
- Myasthenia gravis, a neurological condition which can lead to profound disability and death
- Certain hormone deficiencies (but only those which were recognised in 1968 and were expensive to treat in 1968)
- Anyone who had a fistula (a hole causing body fluids to leak from the urinary system or digestive system onto the skin surface), if that hole was permanent.
In 2009 cancer patients were included, not only for their initial phase of treatment, but potentially on a permanent basis. They are exempt from paying for prescriptions as long as they are having treatment for cancer or for the side-effects of treatment. So, if they develop a coin-sized patch of dry skin where they had radiotherapy and need an emollient cream for that, then they qualify for all their prescriptions to be free forever. Moreover, like all patients who are exempt for one reason, all other prescriptions for unrelated problems are covered by the NHS.
As a doctor, scenarios like the following are quite typical. This morning I saw Mr A, who has high blood pressure and asthma. His medical treatment is essential. Without it he will be unable to work and will be at a much higher risk of strokes, heart attacks and death from asphyxiation.
He is not exempt from prescription charges and must either pay £8.40 for each of the six medications he has to take; or he can pay £109 for an annual season ticket. He is open about his reluctance to use medication regularly because despite his reasonably high income, he has a dependent family and doesn’t feel able to spend the money on medicine for conditions which do not immediately incapacitate him. High blood pressure at this level does not produce any symptoms at all until the stroke or heart attack or kidney failure occurs.
Then I saw Mr B, who also has high blood pressure and asthma, but is also severely obese and has over-taxed his pancreas so he has to take tablets to keep his blood sugar down. His pancreas does produce insulin, but not enough to cope with what he eats, and the fat around his abdomen produces substances which impede the action of his natural insulin. A few years ago he managed to stick to a diet and his blood sugar was normal without medication, but then he resumed over-eating and it went out of control again. He is classified as a type two diabetic, and as a diabetic he can claim all his prescriptions free. All diabetic people are exempt, except those who change their lifestyle and diet in order to control their blood sugar without medication. Over-eating saves Mr B £109 per annum, and he gets other benefits such as free eye checks.
Mr B is not exceptional. Studies have indicated that the majority of people with type two diabetes mellitus could cure their diabetes by restricting food intake.
This injustice has not passed unremarked. In 2008, Professor Ian Gilmore was asked to review the current arrangements with a view to extending exemption to everyone with a chronic medical condition. His report suggests that the current list was illogical and unfair, but he was worried about the cost implications of levelling the playing field, observing that the NHS would lose revenue of £500 million per annum if prescriptions for chronic conditions were dispensed free of charge. Professor Gilmore suggested phasing in the new, less discriminatory system, and used phrases such as “as soon as possible” – but seven years later, no progress has been made.
Professor Gilmore is appropriately cautious. An Ipsos Mori poll from 2008 indicates that in the course of one year, 800,000 UK residents did not collect a prescription because of the cost. One billion NHS prescriptions are dispensed annually, so there would be approximately an 8% increase in the number of prescriptions dispensed if cost were no longer a barrier.
The NHS could be at risk of a successful class action by one of the minorities who suffer in particular from this system. High blood pressure is much more common in certain ethnic groups; for example, about one in three US black people need medication for it, compared to one in four white people. Alternatively a patient group action might ensue, perhaps by people who have asthma and who need to pay for medication throughout their adult life while they are making an active contribution to the NHS, until they reach sixty and qualify for free medication.
The NHS is an expensive luxury, but having seen the consequences of living without a well-organised public health care system, nobody would want to make it unsustainable. The cost of prescription medication is a significant element, so we need a solution which will be more equitable.
If we were to abolish exemptions from prescription charges, the NHS would gain revenue. If we also abolished pre-payment certificates, the revenue would be a significant contribution to the cost of the service. There would be additional savings because the £8.40 item charge does not cover the cost of paying for the medication and the dispensing service. In other words, every prescription not dispensed represents a greater saving than the cost of the drugs. People would no longer collect medications they do not intend to use, whereas when I do home visits and ask about medication, I am frequently introduced to a private pharmacy containing collections of unopened boxes, collected over the years “just in case”.
It would not be fair, of course, that people with chronic conditions would need to pay for medication. Indeed, it was never their choice to suffer those conditions in the first place. However, we are deluding ourselves if we believe we can make life entirely fair. People would still be protected from much of the cost of their treatment, if there continued to be a flat rate charge per item.
Finally, people should be free to prioritise the demands on their budgets. Long-term medications are generally prescribed in quantities to cover a three-month period, so if there were a £10 charge per item, that would equate to less than £1 per week. Some people choose to prioritise their health needs; they manage their diets; take regular exercise; avoid smoking and drinking to excess – and take regular medication as and when required. Others place less of an emphasis on health maintenance, and that is a lifestyle choice which they should be free to make.

Why Europeans really do need American healthcare
Psychiatrist and blogger Scott Alexander has been on a tear lately about the price of pharmaceuticals in America, in particular the EpiPen, a common device used to treat people who have had severe allergic reactions. The EpiPen’s price has been hiked by about 400% since 2007, which left-wing website Vox blames America’s lack of price controls for but Scott blames on America’s cronyish regulation:
Let me ask Vox a question: when was the last time that America’s chair industry hiked the price of chairs 400% and suddenly nobody in the country could afford to sit down? When was the last time that the mug industry decided to charge $300 per cup, and everyone had to drink coffee straight from the pot or face bankruptcy? When was the last time greedy shoe executives forced most Americans to go barefoot? And why do you think that is?
It’s a fascinating piece and worth reading in full.
But what I’m really interested in is a part of his follow-up piece where he looks at rates of pharmaceutical innovation in the US, compared to countries with price controls:
1. Golec & Vernon (2006) say that as a result of European drug price regulation, “EU consumers enjoyed much lower pharmaceutical price inflation, however, at a cost of 46 fewer new medicines introduced by EU firms [over a 19 year period].”
2. Eger and Mahlich (2014) find that among pharmaceutical companies, “a higher presence in Europe is associated with lower R&D investments. The results can be interpreted as further evidence of the deteriorating effect of regulation on firm’s incentives to invest in R&D.”
[…]
So by my count, there are eight-and-a-half studies concluding that price regulation would hurt new drug innovation, and one-half of a study concluding that it wouldn’t. I’ve tried to eliminate all the studies sponsored by the pharmaceutical industry from this list, but I might have missed some.
Scott also cites an impressive-looking RAND Corporation paper which tries to project the consequences of government price-caps in healthcare.
In the short-term, things get better – drugs are cheaper. Great! But in the longer-term, things get worse. Much worse. Innovation declines and life expectancies fall in both the US and Europe.
Which makes me think that, as bad as the US system is in many ways, there’s a very important silver lining. All that money and intellectual property protection create much, much bigger incentives for healthcare innovation in the US than in Europe.
And that allows those of us in price-controlled countries to get something like the best of both worlds: cheap(er) drugs, but lots of research for new drugs, funded by our less fortunate friends in the United States. In a very important sense, it looks as if we’re free riding on American healthcare spending.
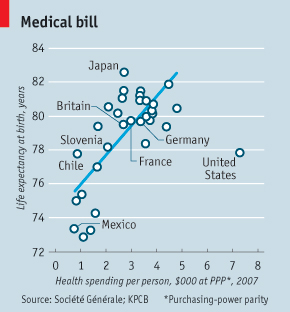
None of which is to say that the US system isn’t a dog’s dinner. Read Scott’s posts to get a flavour of that. But it does make smug posts and charts like the one above, which laugh at the nutty Americans and their wild, wasteful overspending, look quite silly. Without Americans spending all that money on healthcare, those of us living in price-controlled European systems would be living shorter lives, too.